

"I have COVID! What should my kids and I take to reduce chances of severe illness and Long COVID?" (Updated 9/14/24)
I get this question a lot. Here is some info that may help adults & children with COVID.

Here are some of my current best bets for speeding up COVID recovery and reducing the chances of Long Covid. I’m focusing on accessible pharmacological treatments with a good balance of safety, tolerability and (potential) efficacy, based on currently available information. This is not an exhaustive list, but a few select treatments that can, for the most part, be combined together if desired. At the end of each treatment review, I present dosing/brand information for both adults and children. If you just want to see a summary with a sample treatment/dosing schedule, scroll to the end.
NOTE: It goes without saying that REST is incredibly important during and at least 3 months after infection; these picks are not a substitute for good rest and restorative sleep! To start, I include some info on sleep supplements which also may inhibit SARS-CoV-2.
Some of you have messaged me asking where you might leave a tip or donate. I have never collected tips/donations and all my content is free, but now tips are an option by clicking on the “Support me” button below. Thank you so much!😊
SLEEP SUPPLEMENTS
Many have sleep troubles during acute SARS2 infection which very likely impedes recovery and increases the risk of Long COVID. Three sleep supplements that may not only aid sleep but also help reduce illness severity and post-acute sequelae via other mechanisms are listed below.
NOTE: I tend to recommend liquid formulations to allow for flexible dose titration and sublingual administration (in smaller volumes). Sublingual (under the tongue) administration increases systemic absorption, exerts faster onset of action, and limits drug interactions by avoiding first-pass metabolism.
MELATONIN Drops (sublingual immediate release +/- oral time release)
In addition to lengthening sleep duration, some studies in adults suggest 5 to 10 mg daily melatonin improves COVID outcomes, including thrombotic events and mortality.
Melatonin may suppress platelet hyperactivation, microclot formation and even incidence of ischemic reperfusion injury—issues which many Long COVID sufferers experience. Some experts believe that ischemic reperfusion is related to post-exertional malaise (PEM). Relatedly, a recent pilot study (n=65) found that early treatment of 20 mg melatonin once daily for five days improved functional & neurological recovery in patients 30 to 90 days following acute ischemic stroke.
If you’re having trouble staying asleep, consider adding 1 to 5 mg melatonin time release tablets. Start with 1 mg to assess tolerability. I do not recommend taking melatonin for nighttime awakenings.
Adult dosing: KAL drops linked above contain 3 mg per 20 drops. These should help you fall asleep but you may have to experiment with dosing. A lot of people have success with just 0.3 mg sublingually for sleep, but 0.3 mg likely won’t exert many additional benefits at that low of a dose.
For kids age 3+, I recommend staying around 0.3 to 0.5 mg, which would be 2 to 4 drops of KAL. Avoid in children younger than 3 yrs old. Another option is Mommy’s Bliss Kids’ Sleep Liquid, which combines 0.5 mg melatonin with a similar herbal concoction (chamomile, lemon balm, passionflower) as recommended above.
Avoid gummies! Besides being bad for dental hygiene, gummies also involve a host of other issue, which you can read about in this article from Consumer Labs. Again, I prefer sublingual drops administration for superior absorption, faster action, & (generally) cleaner ingredients.
SLEEP Herbal tincture (drops)
Contains valerian, passionflower, chamomile, hops strobile and anise. Shake before use.
Help to fall asleep but not necessarily to stay asleep.
These drops are especially helpful for nighttime awakenings — may help you fall back to sleep.
Chamomile may exert antiviral and antioxidant activity through its beneficial flavonoids luteolin, quercetin and apigenin.
Recently re-branded as kids’ formulation but is same concentration as before when it was marketed for adults. Thus can easily be administered for both kids and adults.
For children over 1 year of age, dosed by weight. I recommend starting around 5 drops for all weights. In my experience, the maximum dose is not typically necessary if dosed sublingually.
Under 25 lbs: 5 to 10 drops maximum
26-50 lbs: 5 to 15 drops maximum
51-75 lbs: 5 to 20 drops maximum
76-100 lbs: 5 to 25 drops maximum
Adult dosing: Bottle recommends 30 drops but that high of dose likely not necessary, especially if administered sublingually. Place 10 drops under tongue and let absorb for a minute or so, then wash down the rest with water if desired. Repeat or titrate up as needed.
For infants as young as 4 months, a similar option is Mommy’s Bliss Organic Baby Bedtime Drops + Immunity Support. It contains elderberry, chamomile, passionflower, and lemon balm. Comes with a dosing syringe, but may be easier to administer with a dropper.
DIPHENHYDRAMINE (last resort for sleep) - updated September 2024
Most people are familiar with diphenhydramine as an antihistamine, but it is also a sigma-1 receptor agonist. Sigma-1 receptor agonists have been shown to exert antiviral activity against SARS-CoV-2 by reducing replication.
An April 2022 study found that histamine facilitates spike protein entry into endothelial cells. Thus it stands to reason that inhibiting histamine with an antihistamine might suppress the S protein from cell entry. Furthermore, a July 2024 in vitro study suggests that histamine receptor H-1 antagonists may reduce SARS2 infectivity in other significant ways. I discuss this in more detail in a later section (“Honorable Mentions”), including some pertinent calculations.
Diphenhydramine’s antiviral activity appears synergistic with lactoferrin according to this in vitro study. The study looks quite exciting at first glance. However, the concentration studied was higher than what is achievable in humans (54.25 µg/mL in study vs 0.066 µg/mL Cmax in humans). Nevertheless, it is possible this combination may exhibit additional benefits. I discuss lactoferrin next.

Liquid formulations like Nytol (UK) or Genexa (US) may be administered by mouth or even under the tongue to optimize systemic absorption.
If you prefer capsules, I recommend dye-free liqui-gels.
Diphenhydramine’s duration of action is around 4-6 hours, so it may help you stay asleep longer than immediate-release melatonin or the herbal concoction, both of which are shorter-acting.
Since diphenhydramine is sedating, I recommend only taking it at bedtime and not around the clock.
Avoid in: ages 65+, glaucoma, Long QT Syndrome, cognitive dysfunction, or those taking other anticholinergic medications (amitriptyline, oxybutynin, hydroxyzine, clemastine, chlorpheniramine, et al). Check with pharmacist if unsure.
Adult dosing: May be somnolent at doses as low as 10 mg but most may need 12.5 to 25 mg at bedtime with a maximum dose of 50 mg. With liquid formulations, one can titrate up or down easily as needed in small intervals.
Children: Avoid use in children under 6 yrs old. Speak with pediatrician before using in kids 6+ for sleep. May cause paradoxical hyperactivity or insomnia.
MY FIVE BEST BETS (in no particular order):
1. NATTOKINASE
Safer and more effective alternative to aspirin? (Updated Sept 2024 for higher dosage recommendation & new study)
Microclots have been reported in both acute COVID and Long COVID. A 2021 study found anomalous amyloid microclots in Long Covid patients comparable to those in acute Covid patients. More recently, an August 2024 study published in Nature concluded that “fibrin drives inflammation and neuropathology in SARS-CoV-2 infection.” Importantly, nattokinase and lumbrokinase have been shown to degrade amyloid fibrils in vitro. These in vitro studies also found that amyloid degradation is pH-dependent and the fibrinolytic activity of nattokinase stops in pH<5 (gastric pH is normally ~2-3).

A study published in Thombosis and Hemostasis uncovered evidence of disordered clotting in Long Covid. Of the 330 patients, 26% had elevated Factor VIII, ranging from 2.1 to 5.1 IU/mL (normal range: 0.5-2 IU/mL), and 18% had elevated von Willebrand Factor (vWF), ranging from 1.7 to 3.3 IU/mL (normal range: 0.5-1.6 IU/mL). Both of these factors help the blood clot, and levels above the normal range suggest a higher risk for thrombosis. Importantly, trials in humans have shown that nattokinase reduces vWF and fVIII within normal ranges. One open-label human trial (n=45) found that nattokinase 4000 FU daily reduced Factors VIII & VII by 17-19% & 7-14%, respectively, after 2 months. A double-blind RCT (n=74) investigated the effects of nattokinase on von Willebrand Factor. Patients took NSK-SD (not enteric-coated) 2000 FU once daily for 8 weeks and on average their vWF reduced by 15%. I suspect that at higher doses with enteric coating, the reductions in vWF and Factors VIII & VII would be even greater.
A 2021 study found sustained pro-thrombotic (clot-promoting) changes in “recovered” COVID patients FOUR MONTHS after hospital discharge: Plasminogen-activator inhibitor type 1 (PAI-1) levels were significantly elevated (0.6 vs 3.15 ng/L, p<0.0001) while plasmin-antiplasmin (PAP) complexes were significantly lower compared with controls. Low PAP and high PAI-1 raise alarm bells for higher blood clot risk. Nattokinase has been shown to degrade PAI-1 and increase PAP. During acute COVID and even in the months after apparent “recovery,” nattokinase may help mitigate cardiovascular damage and/or complications.

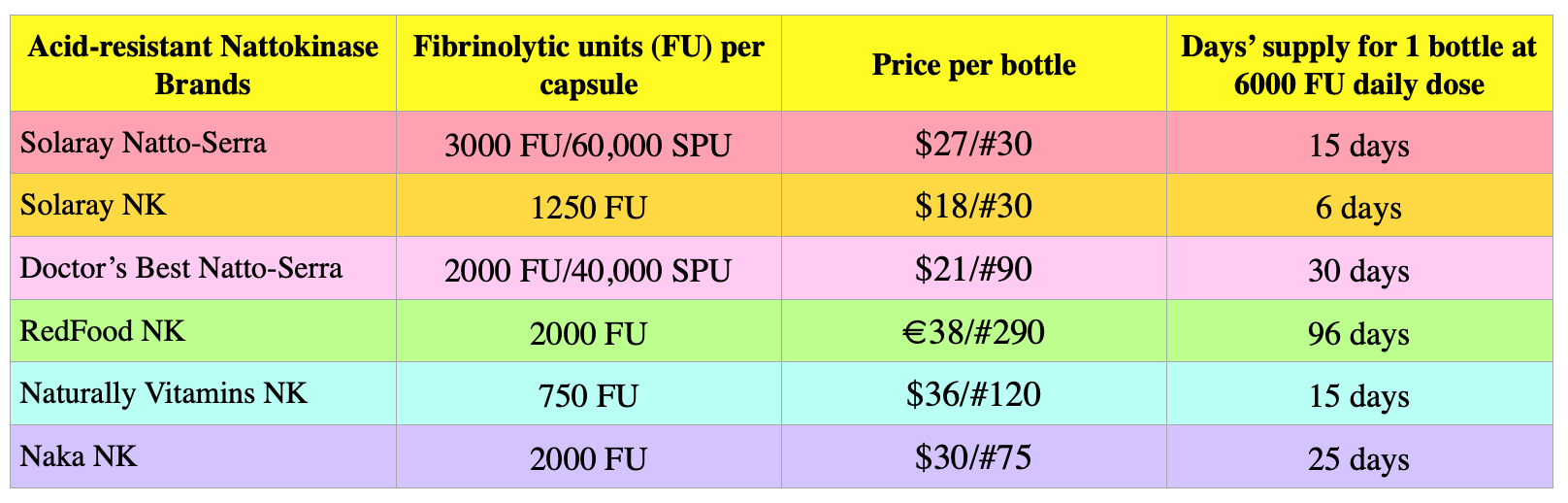
Adults: For preventive measures during acute COVID, nattokinase doses ranging from 2000 to 5000 FU twice daily may be sufficient, but based on my Long COVID surveys and the aforementioned Nature study uncovering fibrin’s pathological in COVID, I suspect that minimum doses of 4000 FU twice daily may be warranted. Dose adjustments may be advised depending on individual’s medical history, risk factors, and other medications. Enteric coating contribute to better absorption and fibrinolytic efficacy. For info on nattokinase potential drug interactions, see my write-up here. Info on lumbrokinase drug interactions is lacking but may be similar to nattokinase. For more info, see my FAQ.
Children: To my knowledge, there have been no nattokinase or lumbrokinase trials in children, but some physicians reportedly have treated children with nattokinase in half doses (~1000 FU daily). I personally wouldn’t recommend nattokinase in children younger than 12 years old, but they could eat natto. Best low-dose brands of supplements are Solaray NK 1250 FU and Naturally Vitamins NK 750 FU.
ALLERGY NOTE: For those with soy allergy or MCAS, consider that nattokinase is sourced from fermented soybeans. Some but not all with MCAS report have reported exacerbations. Healthy Origins makes a soy-free nattokinase but unfortunately it is not enteric-coated and may require higher doses for comparable efficacy. Some with MCAS report better tolerability with lumbrokinase, another fibrinolytic enzyme. More info on lumbrokinase in my FAQ.
2. METFORMIN
Upgraded Sept 2024 from honorable mention to Top 5 Pick
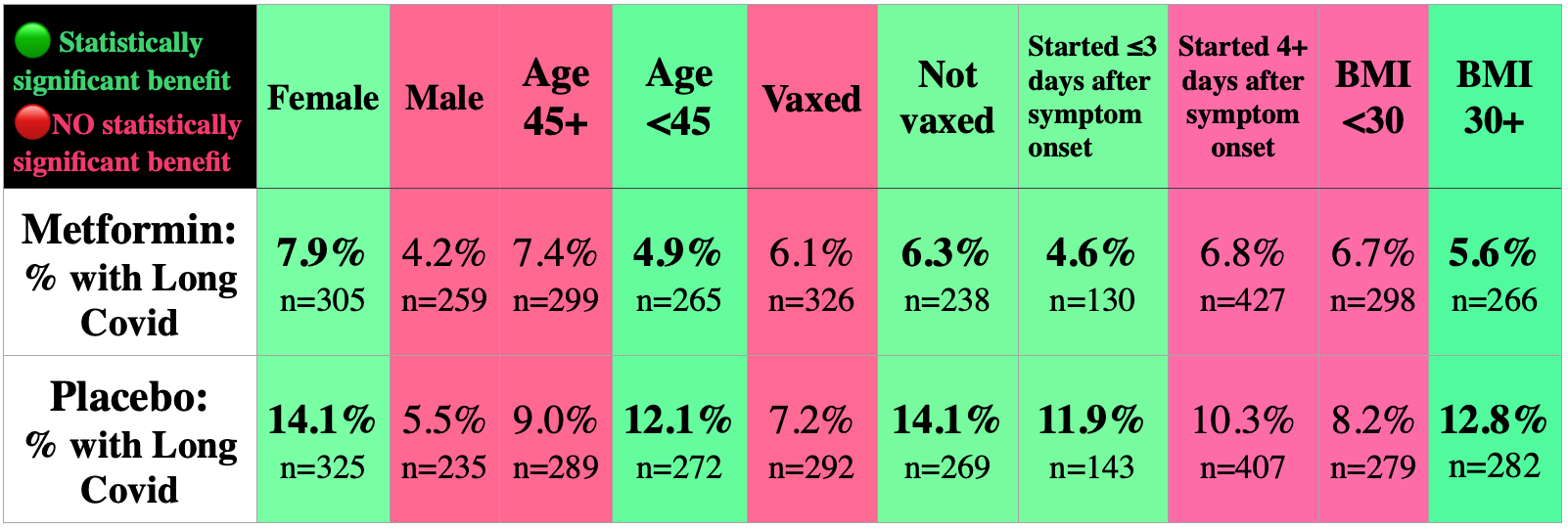
A trial published in May 2024 showed METFORMIN significantly reduced viral load over the course of 10 days, viral load rebound, and progression to Long COVID. In this trial that also investigated ivermectin (3 day course) and fluvoxamine (14 day course), only metformin (14 day course) yielded statistically significant benefits.

To aid tolerability, the metformin dose was titrated up, starting at 500 mg on day 1, then 500 mg twice daily for 4 days; then 500 mg mornings and 1000 mg evening through 14 days. The absolute risk reduction of Long COVID was 4.3%. For those curious, the relative risk reduction is calculated as follows:

Some have expressed concern that development of Long Covid was only a secondary endpoint of the original study whose primary endpoint investigated hypoxemia (≤93% oxygen saturation on home oximetry), emergency department visit, hospitalization, or death. (Results in that study found that none of the three medications prevented the occurrence of any endpoint.) This is a valid concern. Trials are powered for primary endpoints and not for secondary endpoints. Nevertheless, I still suspect that metformin may be helpful in the longer term, especially considering its positive effects on viral clearance (slower viral clearance has been associated with greater risk of Long COVID, particular in women, in this July 2024 preprint).
In summary, a short course of metformin should lower viral load and may help some people reduce their risk of Long Covid. While the study was not specifically powered to assess subgroups, authors noted that certain subgroups seemed to benefit more than others (see chart below). If prescribed, start metformin as soon as possible, within 3 days of symptom onset.
Metformin is a relatively safe prescription medication typically prescribed for type 2 diabetes. However, I wouldn’t recommend it for children as it hasn’t been studied in this population for COVID. Metformin has a low risk of hypoglycemia but does exert significant gastrointestinal side effects, especially diarrhea, nausea, and vomiting. Careful dose titration may reduce these adverse effects. Lactic acidosis is very rare but possible. While metformin may cause vitamin B12 deficiency, it is very unlikely to occur over a short 14-day course. However, one could supplement with B12 if concerned. Discuss metformin with your physician and ask if a standy-by prescription for a 14-day course might be appropriate for you.
One final note: Berberine and metformin share some similarities in several key mechanisms of action. For example, both activate AMP-activated protein kinase (AMPK) and inhibit mTOR. Berberine also has similar dosing and side effects as metformin. Could berberine reduce risk of Long COVID? It is certainly worth studying. However, a big concern is bioavailability—that is, what percentage of the dose reaches systemic circulation and thereby its therapeutic destination? Metformin has good oral bioavailability at around 40-60% whereas berberine’s is well under 1% due to extensive hepatic metabolism, P-glycoprotein efflux and poor intestinal absorption. If you decide to try berberine, combining it with nattokinase might help absorption due through P-gp inhibition. Consumer Labs tested various berberine supplements and their top pick was Solaray brand. I like Solaray’s berberine phytosome “Prosorb” that contains 550 mg of berberine phytosome standardized to 30% berberine HCl.
3. EGCG
EGCG, a potent catechin & antioxidant found in green tea, inhibits both EBV and SARS-CoV-2. This in vitro study found that EGCG inhibits SARS2 replication via inhibition of M-protease—the same enzyme target as Paxlovid—and even more potently via other mechanisms. As can be seen from the images below, even at the low concentration of 1 µg/mL, EGCG appears to significantly reduce coronavirus replication and relative activity of M-protease. But is this concentration achievable in humans??
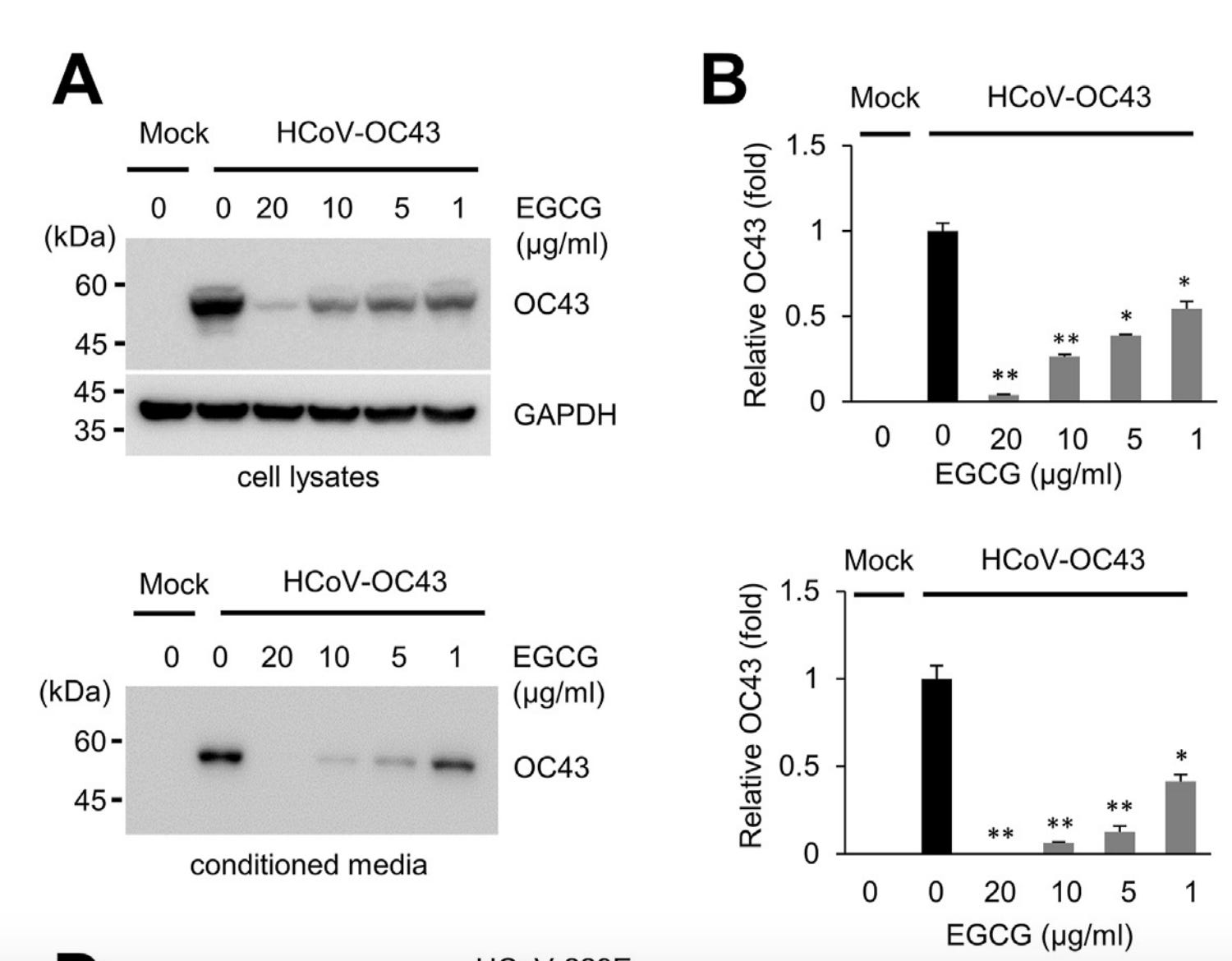
Yes!! After just one single 800 mg dose of EGCG, one pharmacokinetic study found that humans reached a mean maximum concentration of 2.3 µg/mL, and after 10 consecutive days, that increased to 2.8 µg/mL. This may reduce relative activity of M-protease by up to 25%! No serious adverse events or any other clinically relevant adverse events were reported. However, one of the twelve participants did show elevated ALT which resolved on its own within 2 weeks.


So is 800 mg considered safe? Sources say yes, but don’t go any higher than that. In 2018, the European Food Safety Authority presented its scientific opinion on the safety of green tea catechins and they concluded that green tea infusions in typical daily doses of up to 866 mg EGCG are generally considered to be safe, while EGCG supplements in doses above 800 mg/day may increase liver enzymes. Drinking several cups of EGCG-rich green tea daily plus EGCG supplements to target 800 mg during acute infection and up to 10 days may very well reduce viral load and , thereby attenuating or preventing progression to Long Covid.
Drug interactions: If you opt to take a higher dose of EGCG (≥300 mg), keep in mind some drug interactions are possible, but it’s unknown how clinically relevant they might be. EGCG is a CYP3A4, CYP2C9 and CYP1A2 inhibitor, so if you are taking any medications that are moderate to strong substrates of these enzymes, consult with your pharmacist or physician about potential dose adjustments. Some possible (but not necessarily clinical relevant) interactions with EGCG are listed in the table below:

You may search DailyMed for your medication(s) and then scroll down to Drug Interactions. If your medication is involved in clinically significant CYP interactions, it will say so there. For example, here is what ivabradine’s drug interaction section looks like:

Adults: Maximum dose 800 mg once daily for 10 days, then decrease to 200-400 mg once daily for 8-12 weeks. The chart below shows well-reputed brands of teas and supplements with higher EGCG content. I favor Teavigo because it has been used in clinical trials, but all other brands have been tested and approved by Consumer Labs. If I were to dose aggressively during acute illness, I might take 6 Teavigo capsules (700 mg EGCG) plus an additional cup or two of green tea to yield 800 mg EGCG. Please note in the study discussed above, the participants took 800 mg in one single dose on a completely empty stomach: they took first thing in the morning and did not eat for 4 hrs thereafter. They also only took this high dose for 10 days.
Children: EGCG in FontUp chocolate beverage was trialed in children age 6 to 12 years old with similar adverse effect profile to placebo. Dose was 10mg/kg/day in two divided doses which came out to 1 to 2 satchets total per day. Treatment continued for 6 months. However, this product seems difficult to procure. Older children aged 13-18 years old may drink decaffeinated green tea or take 10 mg/kg EGCG (max 500 mg daily in those over 50 kg) for up to 5 days.

TIPS: To improve absorption, drink green tea or take EGCG supplement on an empty stomach along with ≥10 mg of vitamin C. Vitamin C reportedly increases absorption of gallated tea catechins including EGCG “extraordinarily.” You can simply sprinkle a tiny bit of vitamin C powder directly into your water or tea or supplement with <100 mg (~1/4 tsp or 1.25mLs) of liposomal liquid vitamin C. I don’t recommend a higher dose of vitamin C on an empty stomach as it could cause nausea or even vomiting. Unfortunately, higher doses of EGCG also may cause nausea. These organic green teas from Japan are excellent quality and may be better tolerated. This mouse study found that fish oil also improved EGCG absorption; moreover, fish oil and EGCG synergistically inhibited cerebral amyloid β deposits which are found in Alzheimer's Disease. Thus it’s possible this combination could be neuroprotective.
4. LACTOFERRIN
Lactoferrin is an iron-binding glycoprotein with immunomodulating properties. It has been studied in both adults and children and has a good safety profile in all age groups, even infants. A 2020 RCT (n=290) found that lactoferrin significantly reduced duration of total infectious diseases compared to placebo. A 2021 meta-analysis backed up these results further.
This small study (n=92) compared three groups of COVID patients: 1) those treated with liposomal lactoferrin, 2) patients with no treatment, and 3) patients treated with the HIV antiviral Kaletra (lopinavir + ritonavir) plus [hydroxy]chloroquine. Those treated with lactoferrin showed both clinically & statistically significant improvements over the other two groups, including shorter time to test negative, superior symptom resolution, and reductions in ferritin, D-dimer and IL-6. See results compiled in chart below. Note that patients in the lactoferrin group achieved symptom remission across almost all symptoms monitored, in striking contrast to those taking Kaletra plus [hydroxy]chloroquine.

Another trial, COVID-LF, found no difference in COVID symptom severity between placebo and lactoferrin groups. Importantly, however, that study was not powered to assess this secondary endpoint—in other words, the sample size was not large enough to determine a difference if there was indeed one. Furthermore, the study was stopped early (63 days vs the planned 90) due to the availability of COVID vaccines.
It is well-established that COVID often leads to reactivation of latent pathogens. As a result, for some, Long COVID may actually involve symptoms caused by these reawakened pathogens. Lactoferrin may exert action against not only SARS-CoV-2 but also many other viruses and bacteria via several routes as noted below.
competes with SARS-CoV-2, HSV-1, HPV, and even HIV for cell receptor occupancy — namely HSPGs on cell membranes — thereby blocking viral docking and entrance into cells.
prevents iron utilization by many harmful pathogens—including SARS-CoV-2— which need iron for replication/growth
promotes innate immunity via natural killer cell recruitment
enhances humoral immunity by stimulating B and T cells (so if you’re getting a booster, lactoferrin may provide an added “boost” to the booster!)
may diminish cytokine storm
improves gut microbiome

Note that lactoferrin is better absorbed with enteric coating and on an empty stomach. Unfortunately it is difficult to find enteric-coated lactoferrin. Liposomal formulations may also yield a more beneficial immunmodulatory response according to this small RCT comparing liposomal vs non-liposomal lactoferrin in ten healthy men. The only liposomal formulations I found can be purchased here, here, and here, but they are quite expensive. Lactyferrin Forte Defense is the same liposomal formulation used in clinical trials, but a 250 mL bottle contains just 64 mg lactoferrin per 20 mLs and would require more than one bottle per day to reach the desired total daily dose of 1000 mg! Since this is impractical and very expensive, another option may be to empty the contents of two 250 mg capsules of Jarrow’s and mix with liquid sunflower lecithin (phosphatidylcholine) or a small volume of liquid liposomal vitamin C to improve absorption. Even better, one could purchase empty delayed release capsules and transfer the contents of the lactoferrin inside these capsules.
Adults: Recommended dosing is 500 mg twice daily on an empty stomach for 28 days, then may reduce to 500 mg once daily or 250 mg twice daily for another 8 weeks minimum.
Children: 400 to 600 mg daily have been used in children (see case series below). Lactyferrin Forte Defense is a flexible option for younger kids who cannot swallow pills. For babies and toddlers, another option is Jarrow Baby’s Big Support, but it is very expensive ~$42) with only 30 doses at 100 mg per dose. One could attempt mixing in an additional 250 mg from the capsule of Jarrow’s lactoferrin capsules. Another options is to simply mix Jarrow’s 400-500 mg with milk as done in a recent case series described below. Adding a few drops of lecithin may improve absorption further, as cited above. Ask your pediatrician if appropriate and cite this small case series that treated persistent post-COVID GI symptoms in a baby and 6-yr-old child with lactoferrin. The contents of lactoferrin capsules were emptied and dissolved into water or milk for the boy (600 mg) and the 11-month-old baby (400 mg). Course of treatment was 90 days. The boy’s GI symptoms completely resolved after 2 weeks on lactoferrin, while the baby’s symptoms improved “considerably” after just 1 week. Anecdotally, authors also reported that while the 6-yr-old was on lactoferrin, he and his family (mom, dad, & baby) were all infected with coronavirus again, but the boy was the only family member who did not experience any symptoms.
5. PAXLOVID (Updated Sep 2024)
Data is mixed on Paxlovid. It appears there is benefit in older males (mean age 62 yrs) with at least 1 risk factor for progression to severe COVID, but the data in other populations is less certain. Nevertheless, let me be clear: I still would take it if given the option (and ideally, a 10-day course).
As mentioned above, one cohort study based on prescription records showed favorable results: Paxlovid reduced progression to Long COVID by 26% (see below) in a population including higher risk & mostly male patients (see below).

However, a subsequently published survey-based study in 66% women found no statistically significant differences between Paxlovid/No Paxlovid groups (see below).

Some pertinent information comparing the two studies is shown in my table below:

One advantage of Study #2 is that it includes more women (66% compared to an only 14% men in Study #1). Since women are twice as likely as men to experience Long COVID, it is crucial that women are represented adequately in these studies. However, those included in Study #2 were older (mean age 62 in Paxlovid group), with pre-menopausal women under-represented. This is noteworthy because sex hormones likely contribute to differences in outcomes, and Long COVID prevalence tends to be greater in younger ages:

Another downside of Study #2: the symptoms surveyed were for acute COVID and not specifically for Long COVID. For example, two of the most common symptoms in Long COVID (brain fog and post-exertional malaise) were NOT included in the survey. This could have skewed the results toward no difference. Furthermore, only 353 participants who took Paxlovid answered the survey (186 women and 170 men). A larger-scale study including all ages and Long COVID symptoms surveyed is warranted. In the meantime, I do not consider this study sufficient to rule out Paxlovid’s potential utility in reducing risk of Long COVID.
Of note, the August 2024 "STOP PASC" RCT investigating a 15-day course of Paxlovid showed no significant improvements in Long COVID symptoms in Long COVID patients.
Children: Neither study described above included children. Furthermore, Paxlovid is not authorized for use in children younger than 12 years old or weighing less than 40 kg (88 lbs).
HONORABLE MENTIONS:
EPA or IPE, Palmitolyethanolamide,& Antihistamines
1. EPA (omega-3 fatty acid)
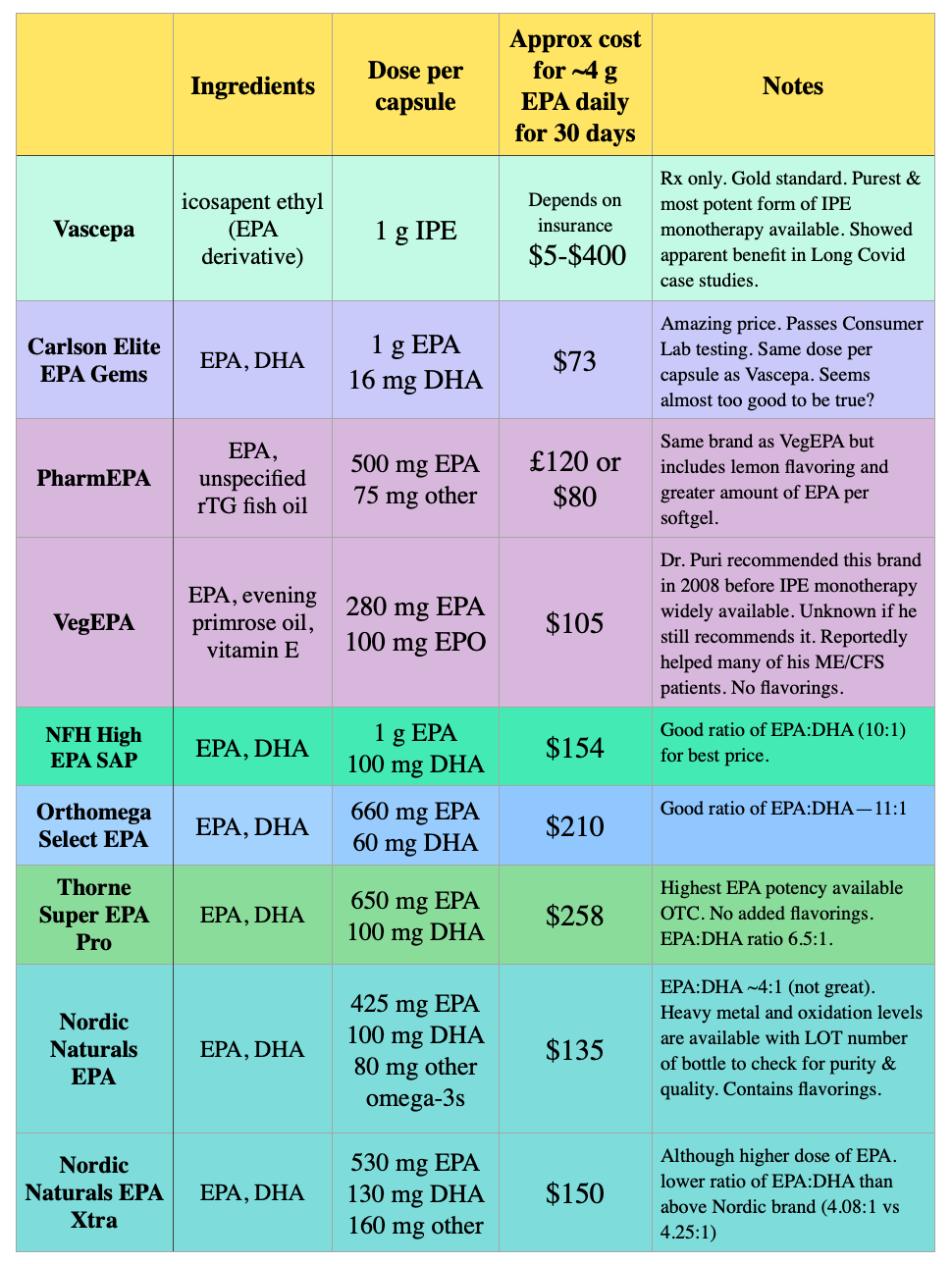
My last article delved deeply into EPA: if you haven’t ready this post yet, check it out. Currently high-dose EPA — or more accurately, the EPA derivative IPE — is being investigated for its use in preventing SARS-CoV-2 or reducing severity of COVID. The authors of this study noted that “preclinical data and clinical observations suggest that IPE may have pleiotropic effects including antiviral and anti-inflammatory properties that may prevent or reduce the downstream sequelae and cardiopulmonary consequences of viral [upper respiratory infections].” Anecdotally, one doctor reported to me that none of his ~160 acute COVID patients who took Vascepa (a high-dose brand of IPE) developed Long COVID.
Adults: Take at least 500 mg to 2 g twice daily with the fattiest meals of the day to increase systemic absorption. Please be advised that in doses above 1 g, risk of atrial fibrillation & flutter slightly increases, especially in those with history of AFib or AFlutter. If you have a history of AFib or AFlutter, avoid use, or speak with your doctor before starting.
Children age 12-17 yrs: Varies between individuals, but a maximum dose of 500 mg twice daily with fattiest meals of the day may be a good rule of thumb. Avoid in children with heart arrhythmias and speak with pediatrician first.
Children age 6-11 yrs: Varies between individuals, but a maximum dose of 750 mg total daily dose with the fattiest meal(s) of the day may be a good rule of thumb. Consult with pediatrician. Multiple trials have investigated EPA and EPA/DHA combos in children as young as 5 years old with good tolerability and safety. The doses studied were as high as 2 g daily with average doses hovering around 500 to 800 mg daily. Avoid in children with heart arrhythmias and speak with pediatrician first.
Children age 2-5 yrs: Consult with pediatrician. A maximum of 300 to 500 mg total daily dose with the fattiest meal(s) of the day may be a good rule of thumb. It is difficult to find palatable liquid EPA-dominant formulations for children. Most are DHA-only. Barlean’s Omega Pals is one possibility but the ratio of EPA:DHA is less than ideal at 3:2. Another albeit less convenient option involves drawing up milk or child’s favorite juice in a 5 mL dosing syringe (you can get these for free at most local pharmacies if you ask), then carefully poking a hole into the EPA softgel (VegEPA or PharmEPA may be perfect options dose-wise) and squeezing the oil into the syringe. Then administer to your child immediately. This ensures they get the full dose. Alternatively, you could skip the dosing syringe and directly add the oil from the softgel to a small volume of your child’s favorite smoothie. Try this approach only if you are confident your child will drink it within a few minutes of preparation to avoid fish oil oxidation. You could also add a few drops of lecithin to aid absorption further. Avoid in children with heart arrhythmias and speak with pediatrician first.
2. Palmitoylethanolamide (PEA)
In vitro & animal studies have shown many promising features of PEA. Perhaps most importantly, PEA binds coronavirus S protein and dismantles lipid rafts used by SARS-CoV-2 for viral entry. Another in vitro study found that PEA reduced SARS-CoV-2 binding to ACE-2 receptors by 50% at 10µM and SARS-CoV-2 entry into cells at concentrations as low as 1 µM. But is that concentration reached in humans? Unfortunately, even a 1.75x more bioavailable formulation known as Levagen only reached a maximum concentration of 0.015 µM in adults per my calculations:

Nevertheless, a double-blind RCT found that compared to placebo, PEA reduced several inflammation biomarkers in non-hospitalized COVID patients. One of those biomarkers was P-selectin, a cell adhesion molecule expressed on activated endothelial cells and platelets.
Along with other mast cell stabilizers, PEA may be a good supplement to prevent mast cell activation syndrome (MCAS), a syndrome that seems to occur in many Long COVID sufferers and causes a host of troubling symptoms, including food intolerances, heart palpitations, brain fog, and hemostatic disruptions. While those with pre-existing MCAS may be predisposed to developing Long COVID, it also may be true that SARS-CoV-2 infection triggers new onset MCAS. This pre-COVID study found that PEA and luteolin can “work synergistically to reduce mast cell-mediated toxicity and elicit neuroprotection.” A Long COVID study found that PEA in combination with luteolin improved olfactory function and memory. Several human trials have found that PEA benefits Long COVID patients by attenuating neuroinflammation.
Adults: Doses used in Long COVID clinical trials were around 600 to 1200 mg total daily dose. Reputable brands include Mirica, Normast, Glialia, and Levagen. Take with fattiest meal(s) of the day to optimize absorption.
Children: PEA has been studied in children in ages as young as 8 years old and has shown good tolerability at an average dosage of 40 mg/kg/day (maximum 600 mg/day).
3. Antihistamines
Most are already well-aware of the H-2 blocker famotidine’s ostensible benefits in acute COVID, but a more recent research article published July 2024 in the American Society of Microbiology also found in vitro antiviral activity against SARS-CoV-2 elicited by H-1 receptor blockers as well.
Famotidine: In this small RCT (n=56), rate of COVID symptom resolution but not time to symptom resolution was significantly improved with the H-2 blocker famotidine: around 50% reduction of overall baseline symptom scores was achieved at 8.2 days (95% CI: 7 to 9.8 days) with famotidine and 11.4 days (95% CI: 10.3 to 12.6 days) with placebo. Recall the dose in this study was 80 mg three times daily (240 mg total daily dose) which is sixfold higher than the typical dose of 20 mg twice daily (40 mg total daily dose).
H-1 blockers: I discussed the H1-blocker diphenhydramine earlier in the Sleep section and mentioned I would discuss this topic further later. That time is now. In vitro studies (2021 study, 2024 study) have found that histamine receptor H-1 (HRH1) helps SARS-CoV-2 infectivity by binding to the viral spike protein, acting as an alternative receptor for SARS-CoV-2, and synergistically enhancing hACE2-dependent viral entry. Thus it stands to reason that H-1 blockers can bind competitively to these sites, blocking viral entry. Indeed, this was found to be the case, with OTC drugs like loratadine (IC50=1.687 µM), diphenhydramine (IC50=2.1 µM) and azelastine (IC50=2.387 µM) boasting some of the lowest IC50 values.
The IC50 values determined in the July 2024 study are half-maximal inhibitory concentrations: the drug concentration required to inhibit SARS-CoV-2 by 50%. Are these values realistically achieved in humans? To find out, I looked up the reported Cmax (maximum concentration) values of loratadine, diphenhydramine and azelastine in humans, converted them to µM via their molar masses, and compared them to the study’s IC50. The results are shown in the chart below.
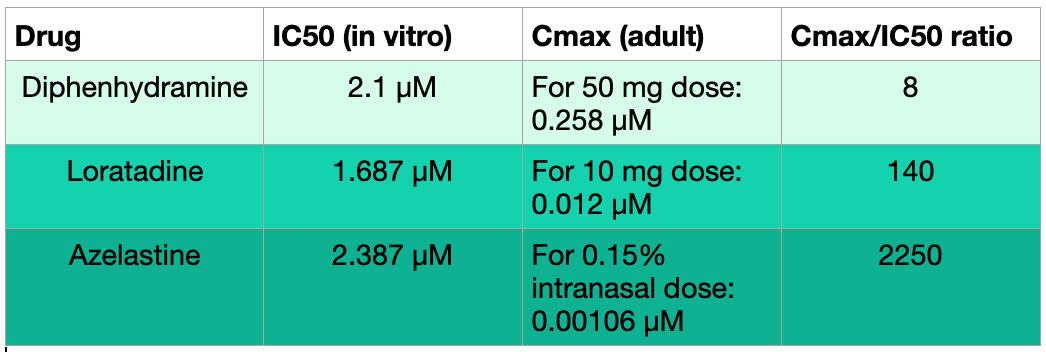
Out of the three drugs above, diphenhydramine 50 mg most closely reaches the concentration required in vitro to inhibit SARS-Co@-2 by 50%. The low Cmax values across all three medications compared to the study’s IC50 values do not mean these medications have no value in COVID. In fact, an electronic health records study from Dec 2020 found that “usage of diphenhydramine, hydroxyzine and azelastine was associated with reduced incidence of SARS-CoV-2 positivity in subjects greater than age 61.” Considering this along with other studies —recall the synergistic combination of lactoferrin + diphenhydramine, for example—this class of medications deserves an Honorable Mention.
Personally, I am not particularly enthusiastic about blanket antihistamine treatments for everyone because I think they are tricky to dose. While some level of inflammation is needed to stave off infection, too much inflammation can be harmful, and it’s difficult to achieve that perfect balance of just the right amount. It may vary substantially between individuals. Therefore, I think it’s best to carefully consider histamine blockers on a case-by-case basis. In children under 6 years old, please consult with your pediatrician regarding potential antihistamine usage and dosage.
SUMMARY
If one wanted to take all/most of the treatments above, here is how I might do it. These are ADULT doses below. Important: this is not medical or pharmaceutical advice. This is based on current available research as of September 2024 and on my opinions as a healthcare professional.
Days 1 - 5 for those who take Paxlovid:
1 hr before breakfast: 1 cup of green tea with ≥10 mg vitamin C
Also may gargle green tea with or without honey
Paxlovid as prescribed
EPA or IPE 1-2 g twice daily with fattiest meals of the day
Melatonin sublingual drops
(if prescribed) Metformin 500 mg with breakfast and 1000 mg with dinner (titrate up) x 14 days
PEA 600 mg twice daily with meals
(if desired) Famotidine 80 mg three times daily and/or OTC H-1 blocker (example: loratadine 10 mg once daily)
Optional: Saline nasal rinse and/or CPC mouthwash
CPC mouthwash reduces salivary viral load and may reduce transmission to others. It’s unlikely that CPC mouthwash reduces Long COVID risk.
Note: Many have asked about taking nattokinase with Paxlovid. The reason I don’t include nattokinase in combination with Paxlovid is due to a possible drug interaction via an efflux protein called P-glycoprotein. Hypothetically, the interaction could increase levels of Paxlovid and thus worsen side effects, but this hasn’t been studied in humans.
Day 6 (or Day 1 if no Paxlovid): at least 4 weeks, preferably 8-12 weeks, except as noted:
>1 hr before breakfast (empty stomach):
1-2 cups green tea
ideally with ≥10 mg vitamin C to improve absorption
Lactoferrin 500 mg
Nattokinase 2000-4000 FU (4000 FU preferred if tolerated)
EGCG capsules
Not to exceed 800 mg total daily dose including tea
800 mg daily studied for treatment duration of 10 days. Since 800 mg is the max doses and liver enzymes could increase with longer administration, recommend dose decrease to 200-400 mg after 10 days.
Please note this may cause nausea in some - advise to start with just 1 capsule to test tolerability
Do not combine with famotidine! It will likely reduce absorption of EGCG due to increased gastric pH. Separate by at least 4 hrs.
(If desired) Saline nasal rinse
With breakfast:
(if prescribed) Metformin 500 mg (14 days total)
(If desired) H-1 antihistamines and/or famotidine
With lunch:
EPA or IPE 500 mg to 2 g
Take at lunch or breakfast — whichever meal is fattier.
PEA 600 mg
With dinner†:
EPA or IPE 500 mg to 2 g
total daily dose not to exceed 4 grams
Vitamin C** 1000 mg
(if prescribed) Metformin 1000 mg (14 days total)
PEA 600 mg
≥2 hours after dinner OR 1 hr before bed (whichever is farther from food and/or more convenient):
Lactoferrin 500 mg
Nattokinase 2000-4000 FU
Bedtime (#1-#4 optional for insomnia):
Melatonin time-release 1 to 5 mg
doses ≥5 mg for antiviral benefit
Melatonin sublingual drops 0.3 to 3 mg
2-8 drops for sleep, 20+ drops for antiviral benefit
SLEEP drops titrated as needed
Diphenhydramine 10 to 25 mg last resort for insomnia in those for whom no contraindications
(If desired) famotidine and/or H-1 antihistamine (the latter not necessary if already taking diphenhydramine for sleep)
(If desired) Saline nasal rinse
†For those taking CoQ10 or Ubiquinol for mitochondrial support, take it with dinner (or fattiest meal) to improve absorption. Doses above 200 mg appear to be more beneficial and well-tolerated in Long COVID per my treatment survey, and a similar dose range could be helpful in acute COVID.
**I am aware of the L-arginine + liposomal vitamin C trials. I have some reservations about L-arg during active infection so did not include it here. If you plan to take L-arg, empty stomach is best. L-citrulline seems to be better absorbed and could be more effective, although it hasn’t been studied in COVID or Long COVID.
Are you aware of ConsumerLabs.com, a phenomenal subscription resource for summaries of the literature on every imaginable supplement and evaluations by quality & brand of many products? Whenever a doctor suggests a supplement to me, it’s the first place I go.
If you don’t have access to it, could I gift you a one year subscription, which I think would be helpful in your research?
I am wondering if there'd be any significant changes to the protocol if one can't access paxlovid (E.g. use nattokinase from day 1?) Paxlovid is out of reach for most of us in Europe unfortunately. Also curious what you think of the claims that curcumin, quercetin resveratrol have 3CLpro-inhibition effects/can they be added when using this protocol?